


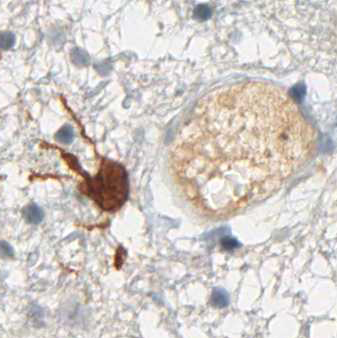

Figure: Immunohistochemistry of a bone marrow biopsy with anti-IDH1 R132H clone H09: Acute myelomonocytic leukemia (AML M4). (Picture courtesy of Professor Harald Stein, Pathodiagnostik Berlin, Berlin, Germany)
A few years back next generation sequencing of whole genomes from acute myeloid leukemia (AML) samples identified new mutations in the IDH1 and IDH2 gene. The mutations occur in 15-20% of newly diagnosed AML patients. IDH1/2 mutations have first been identified in gliomas and researchers wondererd how such mutations could promote malignant transformation. An important next step for understanding the contribution of IDH1 mutations to the transformed phenotype was the discovery that the amino acid substitutions in IDH mutants lead to the generation of the 2-HG “oncometabolite”. The conversion from normal a-KG to 2HG does not only prevent normal catalytic activity but results in a new function, which alters the energy balance of the Krebs cycle by competitive inhibition of dioxygenases. This leads to epigenetic reprogramming blocking diffentiation and contributing to a transformed phenotype. Very soon these mutant enzymes have been considered as clinical targets to reverse their metabolic effect. A breakthrough was presented at the 2014 EORTC-NCI-AACR Symposium on Molecular Targets and Cancer Therapeutics: The IDH1 inhibitor AG-120 shows very promising evidence for clinical activity in AML patients with IDH1 mutation. This IDH1 inhibitor together with an IDH2 inhibitor are also being studied in patients with glioma and data expected to be presented at a medical conference in 2015.
Clinical detection of mutants by sequencing is costly, technically difficult, relies on high quality DNA and often suffers from limited sensitivity (number of tumor cells in tissue is critical). Therefore it would be helpful if the mutation could be detected more easily. Histopathological data suggest the use of IDH1 R132H immunohistochemistry for clinical detection of IDH1 mutations in AML with the advantage of faster turnaround time, lower cost and the potential to detect even single positive cells.